Want to support free content?
Let us know who you are!
Why am I seeing this?
LearnOncology.ca is a free educational content provider. If you want to support our editors (powered by caffeine and no sleep), fill in the following info to let us know who is using the site. We use cookies to prevent this popup from coming up frequently. Continue using the site if you are happy with this.

By the end of this tutorial, the student should be able to:
The most life-threatening symptom associated with advanced intrathoracic disease is hemoptysis. In patients with hemoptysis, the underlying cause is most often malignancy, infection, or hemostatic abnormalities [1]. The severity of hemoptysis can range from blood-streaked sputum to severe, life-threatening bleeding. In patients with cancer, the occurrence of this symptom requires immediate assessment because of the wide range of possible underlying causes and the risk of rapid clinical deterioration. Life-threatening hemoptysis can be defined as expelling 150 mL of blood over 24 hours, bleeding at a rate of ≥100 mL/hr, or airway compromise or hemodynamic instability, which can lead to asphyxiation or exsanguination [2].
Bleeding from a pulmonary malignancy can result from endobronchial disease or from lesions distal to the airways. Among all causes of hemoptysis, malignancy accounts for a substantial and growing proportion. Bronchogenic carcinoma is the most common cause of life-threatening hemoptysis in patients with cancer over 40. Lung metastases from various primary cancers (such as melanoma, breast, kidney, laryngeal, and colon cancer) are another frequent cause [3, 4]. Treatment-related complications, including those arising from targeted therapies, immunotherapy, and thoracic radiotherapy, can also contribute significantly to hemoptysis [5]. Other factors that increase the risk of hemorrhage include thrombocytopenia, coagulopathy (due to the malignancy itself or its treatment), and radiation- or chemotherapy-induced lung damage [3, 4].
The lungs have a unique dual circulatory system, consisting of the pulmonary and bronchial circulations, each with distinct physiological roles. The pulmonary circulation’s main function is gas exchange and the management of total cardiac output at a low mean arterial pressure (typically 12-16 mmHg) [6]. Pulmonary arteries have thin walls, contain minimal vascular smooth muscle, and do not exhibit the same basal tone as systemic vessels. On the other hand, the bronchial circulation’s main function is to deliver oxygenated blood to the conducting airways, pulmonary arteries and veins, and the supporting structures of the lungs [6]. The bronchial arteries are high-pressure systemic vessels and typically account for only 1% of cardiac output under normal conditions, but can be recruited to supply the systemic circulation during certain pathological conditions [6]. These vessels typically originate from the descending thoracic aorta (most commonly between T5 and T6), although anatomic variations are common. The bronchial arteries form a dual-layered network of adventitial and submucosal plexuses along the airways, ending at the terminal bronchioles, where they form extensive connections with the pulmonary capillaries and venules, termed bronchopulmonary anastomoses [7]. These anastomoses become pathologically significant when pulmonary arterial perfusion is compromised. This triggers a maladaptive process characterized by elevated bronchial arterial flow, vascular hypertrophy, and the development of fragile, thin-walled vessels that are susceptible to rupture into the bronchi and alveoli [8].

The pathophysiology of hemoptysis in patients with cancer reflects a complex interaction between tumour characteristics, surrounding blood vessels, and treatment effects. In primary lung malignancies, bleeding typically arises from the bronchial circulation, which supplies the airways and is prone to neovascularization (development of new blood vessels) in response to tumour growth and invasion [10, 11]. Central, endobronchial tumours are more likely to cause hemoptysis than peripheral parenchymal lesions because of their proximity to major airways and the bronchial vasculature [11]. Mechanisms contributing to hemoptysis include [5, 6]:
90% of hemoptysis cases are due to bronchial artery bleeding from neovascularization and tumour erosion, whereas the remaining cases involve bleeding from the pulmonary and nonbronchial systemic arteries, a distribution that underscores significant differences in the vascular anatomy and pathophysiology of these two systems [8]. The distinction between bronchial and pulmonary artery bleeding is critical because of profound therapeutic differences. Massive hemoptysis has shifted from solely volume-based definitions to functional definitions focused on hemodynamic instability, airway compromise, and physiologic reserve [8].
Bronchial artery bleeding results from compensatory increases in bronchial arterial flow triggered by impaired pulmonary arterial perfusion (e.g., pulmonary embolism, vasculitis, hypoxic pulmonary vasoconstriction) [8]. This increased flow through the bronchopulmonary anastomoses causes vascular hypertrophy, with the vessels subsequently becoming thin-walled and fragile, potentially leading to rupture into the alveoli and bronchi. In inflammatory states, angiogenic growth factors promote neovascularization and the recruitment of collateral vessels from nearby nonbronchial systemic arteries (e.g., internal mammary, subclavian, inferior phrenic, and intercostal arteries), which form fragile connections with the pulmonary circulation that are prone to rupture [8, 13].
Pulmonary artery bleeding follows a distinct pathophysiology, typically resulting from a pseudoaneurysm that forms when the vessel wall is eroded by destruction of the surrounding pulmonary parenchyma (e.g., due to chronic inflammation from malignancy, tuberculosis, or lung abscesses) [8]. Although pulmonary artery bleeding accounts for only 10% of massive hemoptysis, it is clinically significant because these sources are often occult on bronchial arteriography and require specific identification with CT angiography for successful embolization [10].

The clinical presentation and symptom severity depend on several factors: the rate and duration of bleeding, the extent of airway obstruction and pulmonary involvement, the patient’s baseline performance, and any concurrent comorbidities [4]. Patients may present with hemoptysis, along with signs of shock and respiratory distress from underperfusion (e.g., hypotension, tachycardia, central cyanosis, clammy skin, dyspnea, or chest pain). A critical initial step is to confirm true hemoptysis by ruling out blood from nasopharyngeal or gastrointestinal sources.

Specific clinical presentations warrant intensive care admission or referral to a specialty center [8]:
When a patient initially presents with hemoptysis, it is important to quantify the volume and rate of bleeding to determine whether the patient is experiencing life-threatening symptoms.
For non-life-threatening hemoptysis, history and physical examination should focus on determining the etiology. Key historical features to assess include [8]:
An ABC assessment is crucial for determining airway patency and hemodynamic stability [8]. Furthermore, lung auscultation and signs of underlying malignancy are important to assess. Certain physical examination findings may also suggest specific etiologies or systemic disease processes:
Initial diagnostic efforts often need to proceed alongside management [4]. As an initial screen, chest radiography and routine laboratory tests (CBC, hemoglobin, platelets, coagulation studies, type & screen) should be obtained to assess for localized pathology. If the patient is unstable, rigid bronchoscopy can be performed at the bedside. Bronchoscopy and CT angiography should ideally be performed within 12-14 hours of presentation, with CT angiography considered the gold standard for identifying the bleeding source and mapping bronchial arteries for intervention [8]. Additionally, bronchoscopy helps localize and treat hemoptysis using iced saline lavage or topical vasoconstrictors.

Initial management of hemoptysis is to protect the patient’s airway. Intubation is warranted for rapid bleeding, hemodynamic instability, ventilatory impairment, severe dyspnea, or hypoxia [4]. Patients can be placed in lateral decubitus with the bleeding side down to protect the non-bleeding lung. Selective intubation, potentially with a double-lumen tube or mainstem intubation of the healthy lung, can also be used to protect the airway. Bronchoscopy is recommended to localize the source of bleeding. After identification, visible airway lesions can be managed with endobronchial techniques such as argon plasma coagulation, Nd: YAG laser, or electrocautery.
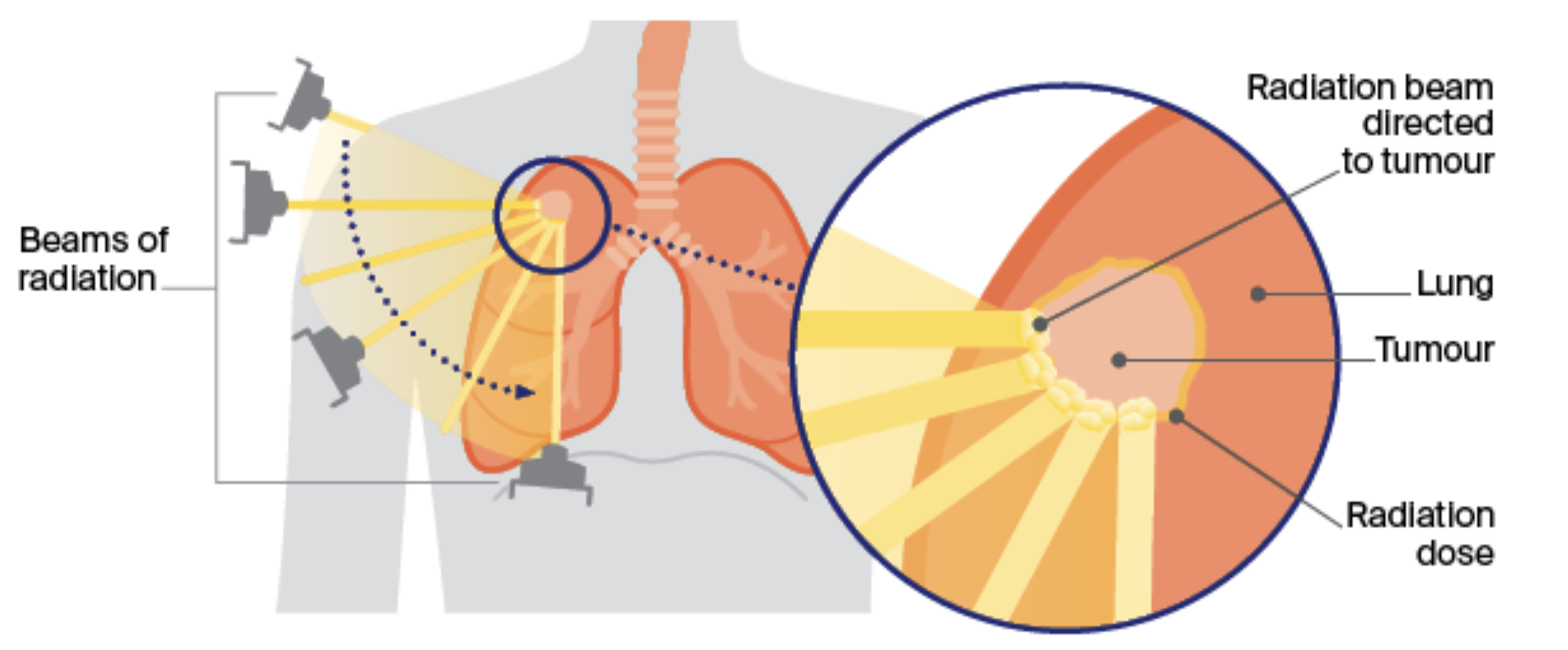
For non-life-threatening hemoptysis, bronchoscopy is still recommended to identify the source of bleeding. For central airway lesions, endobronchial management options are recommended. For distal or parenchymal lesions, external beam radiotherapy (EBRT) is recommended. Bronchial artery embolization can be considered if prior measures are unsuccessful, and systemic therapies, such as antifibrinolytics (e.g., tranexamic acid), may also be used as an adjunct. EBRT has played a major role in palliative therapy, particularly for non-small cell lung cancer (NSCLC). Radiotherapy delivered in a single dose may stop bleeding from a malignant source if the patient is stable enough for imaging and planning [14]. While the precise mechanism is not clear, EBRT is thought to achieve hemostasis through a combination of tumour cell death (reducing tumour burden) and vascular changes (such as thrombosis, endothelial cell damage, and local capillary occlusion). In patients with lung cancer, hemoptysis is palliated in 60-86% of cases, making it one of the most responsive symptoms to radiation therapy [10]. Common palliative regimens include 30-45 Gy for obstructive disease, though shorter hypofractionated courses (17 Gy in 2 fractions or 8-20 Gy in 1-5 days) are preferred for patients with poor performance status, providing similar symptom relief with less time in treatment [15].
Pharmacotherapeutic management of hemoptysis should focus on stabilizing clot formation, correcting underlying systemic issues, and addressing the primary etiology of bleeding. Antifibrinolytic therapy, particularly the use of tranexamic acid (TXA) via nebulized inhaled or systemic routes, is a cornerstone for reducing the duration and volume of non-massive bleeding by inhibiting plasminogen activation [5, 17]. In cases where patients are anticoagulated or have malignancy-induced thrombocytopenia, the focus should shift towards coagulopathy reversal with vitamin K, prothrombin complex concentrates, or platelet transfusions to maintain a safer hemodynamic threshold [18]. Additionally, since infections such as bronchitis or pneumonia are frequently associated with hemoptysis, empiric antibiotic coverage is often initiated. To prevent mechanical dislodgment of clots, antitussives may be prescribed for cough suppression [19]. Historical treatments such as systemic vasopressin and its analogues slow bleeding via vasoconstriction but have largely been phased out due to the risk of cardiovascular complications, in favour of earlier interventional radiology procedures. Bronchoscopic pharmacologic adjuncts can be used if no direct bleeding source is found, such as instilling iced saline to facilitate vasoconstriction. If bleeding persists despite cold saline lavage and topical vasoconstrictors (e.g., epinephrine), topical hemostatic tamponade therapy and arterial embolization should be considered [10].
For life-threatening hemoptysis, studies report mortality rates of 7-30%. In bronchogenic carcinoma, life-threatening terminal hemoptysis from tumour erosion into a blood vessel is rare but carries an extremely poor prognosis, with reported mortality of 59-100% [2]. Predictors of poor prognosis include poor performance status, advanced stage of malignancy, lower hemoglobin levels (each 1-unit decrease increases mortality risk), mechanical ventilation (especially single-lung ventilation), hypotension, cavitation or necrosis, or lung densities involving two or more quadrants on chest X-ray, bleeding from the pulmonary artery, alcoholism, and aspiration of blood into the contralateral lung [20]. Recurrence rates after life-threatening hemoptysis are poorly documented, but some studies suggest higher recurrence after arteriographic embolization than in those who do not require embolization [2].
Follow-up recommendations should consider the volume of hemoptysis at initial presentation and include measures to identify and stabilize the bleeding source and treat the underlying etiology, as this is essential for reducing recurrence [8]. Active treatment of the underlying etiology after achieving hemostasis is crucial to reduce recurrence, as hemoptysis often recurs without definitive treatment of the underlying cause. An important consideration is that bevacizumab (anti-VEGF) is contraindicated in patients with recent hemoptysis and should be discontinued in patients with squamous non-small cell lung cancer, where fatal pulmonary hemorrhage can occur [21]. Surveillance of patients with a history of hemoptysis requires a structured approach that balances routine cancer follow-up with vigilance for recurrent bleeding and disease progression. Some monitoring considerations for individuals with cancer who have a history of hemoptysis include [22]:
Hemoptysis is an oncologic emergency, often signalling primary lung cancer, metastatic disease, or treatment-related complications. The bleeding typically arises from the high-pressure bronchial arterial system, which is prone to neovascularization due to tumour growth. The clinical approach begins with distinguishing true hemoptysis from pseudohemoptysis and determining whether it is life-threatening (defined as ≥150 mL/24 hrs or ≥100 mL/hr), which requires urgent stabilization for airway protection and positioning the patient “bleeding side down” to protect the healthy lung tissue. The diagnostic gold standard for localizing the source is CT angiography, followed by bronchoscopy for direct visualization and initial therapeutic measures such as cold saline lavage. Definitive management includes bronchial artery embolization (BAE) as a first-line stabilization procedure, alongside palliative external beam radiotherapy (EBRT), which is highly effective for malignant bleeding by reducing tumour burden. Pharmacotherapy is a critical adjunct to stabilize clot formation, reverse coagulopathies, or treat any underlying infections, with antitussives used to suppress coughing and prevent clot dislodgment. Surgical resection is generally reserved as a last resort for localized bleeding. Following stabilization, long-term care focuses on surveillance for recurrence and monitoring the progression of the underlying malignancy.
Use your mouse to click through the slides and answer each question in the text box provided.
Note: This case can be completed on an iPad. To do this download the (free) Articulate Mobile Player for the iPad by clicking here.